Cardiovascular Disease
-
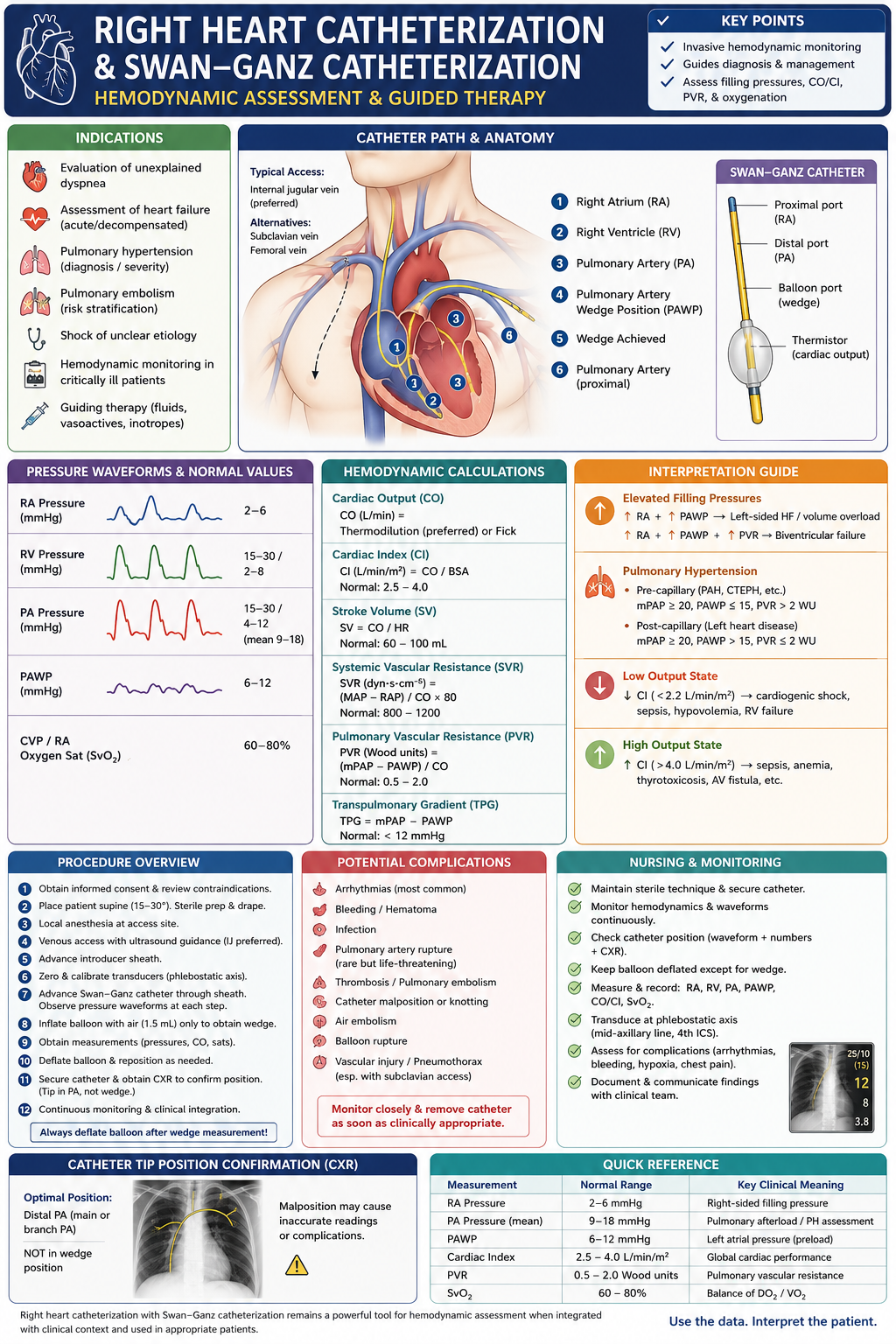
Right Heart Catheterization and Swan-Ganz Hemodynamic Assessment
A clinician-focused review of right heart catheterization and Swan-Ganz catheterization, including indications, catheter positioning, pressure waveforms, cardiac-output measurement, pulmonary hypertension classification, shock profiles, complications, and common interpretation errors. Right heart catheterization, or RHC, provides direct measurement of right-sided and pulmonary hemodynamics. It remains the reference standard for confirming pulmonary hypertension, differentiating pre- from post-capillary physiology,…
-
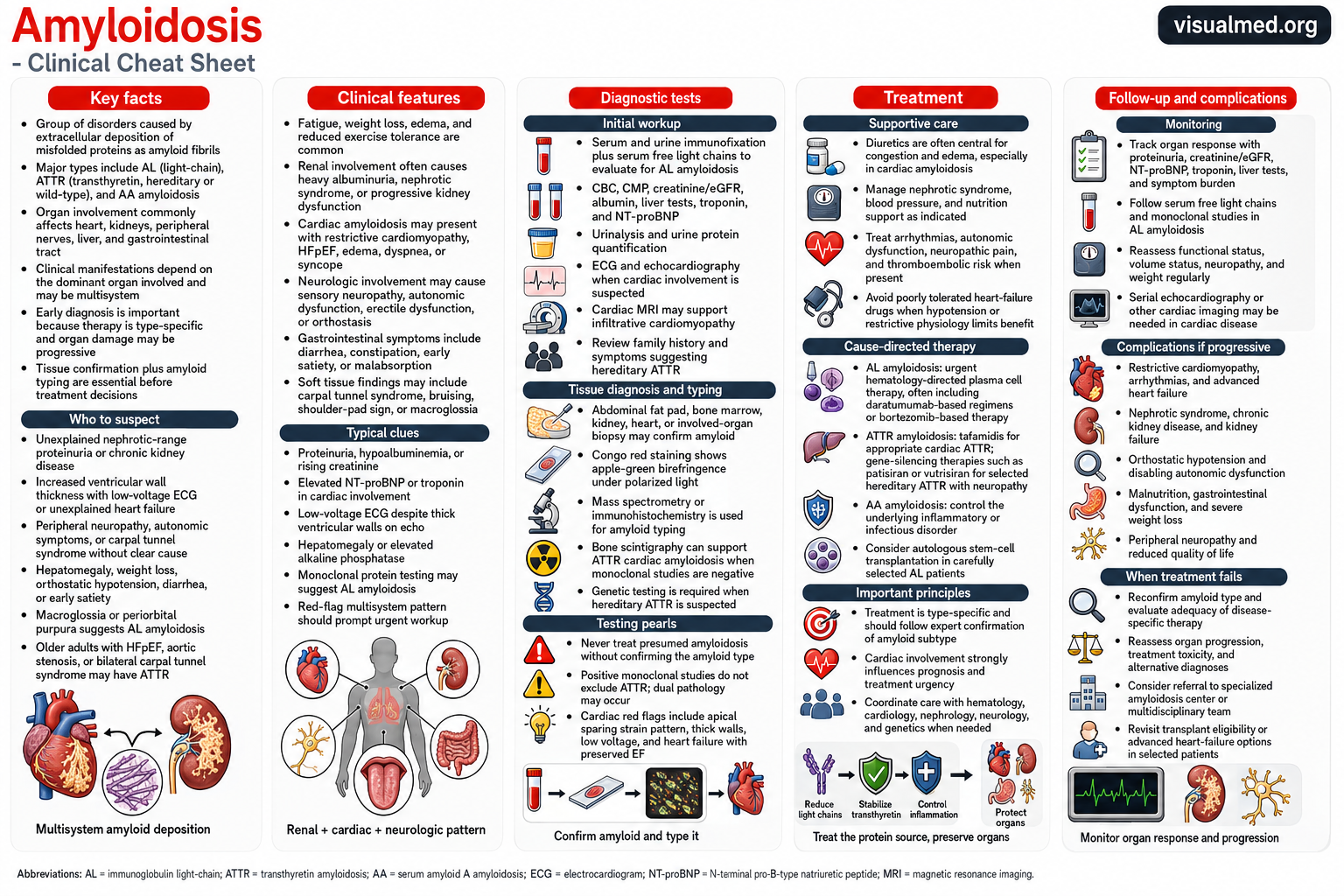
Amyloidosis: Recognition, Diagnosis, and Treatment Clinical Cheat Sheet
Amyloidosis comprises a heterogeneous group of disorders characterized by extracellular deposition of misfolded proteins as amyloid fibrils. The clinical phenotype depends on the precursor protein, the organs involved, and the extent of tissue deposition. The most important systemic forms encountered in clinical practice are immunoglobulin light-chain amyloidosis, or AL amyloidosis; transthyretin amyloidosis, or ATTR amyloidosis;…
-
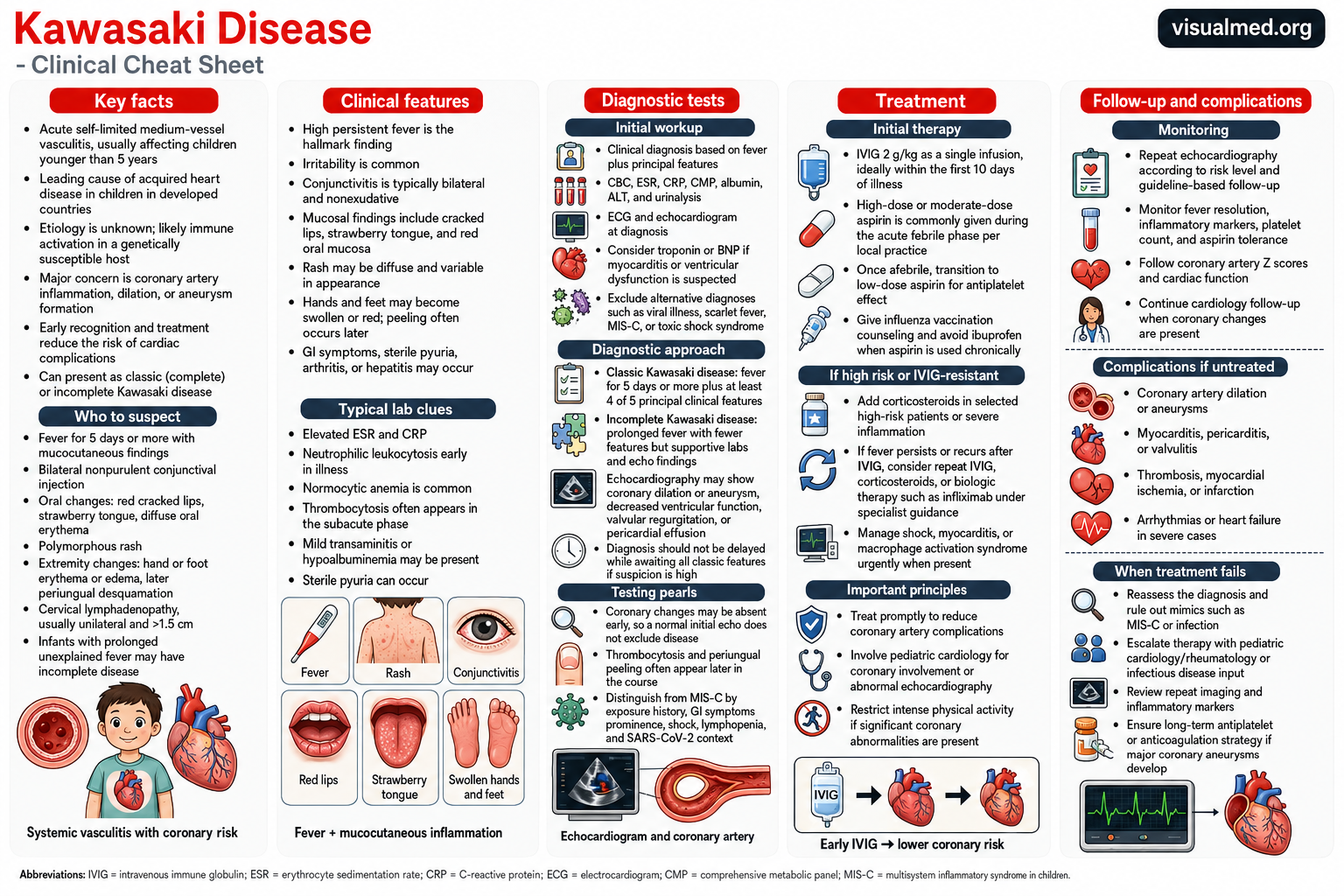
Kawasaki Disease: Clinical Features, Diagnosis, Treatment Cheat Sheet
Kawasaki disease is an acute inflammatory illness that primarily affects infants and young children. It causes inflammation of medium-sized blood vessels throughout the body, with the coronary arteries being the most clinically important vessels involved. Most cases occur in children younger than five years. Kawasaki disease is a leading cause of acquired heart disease in…
-
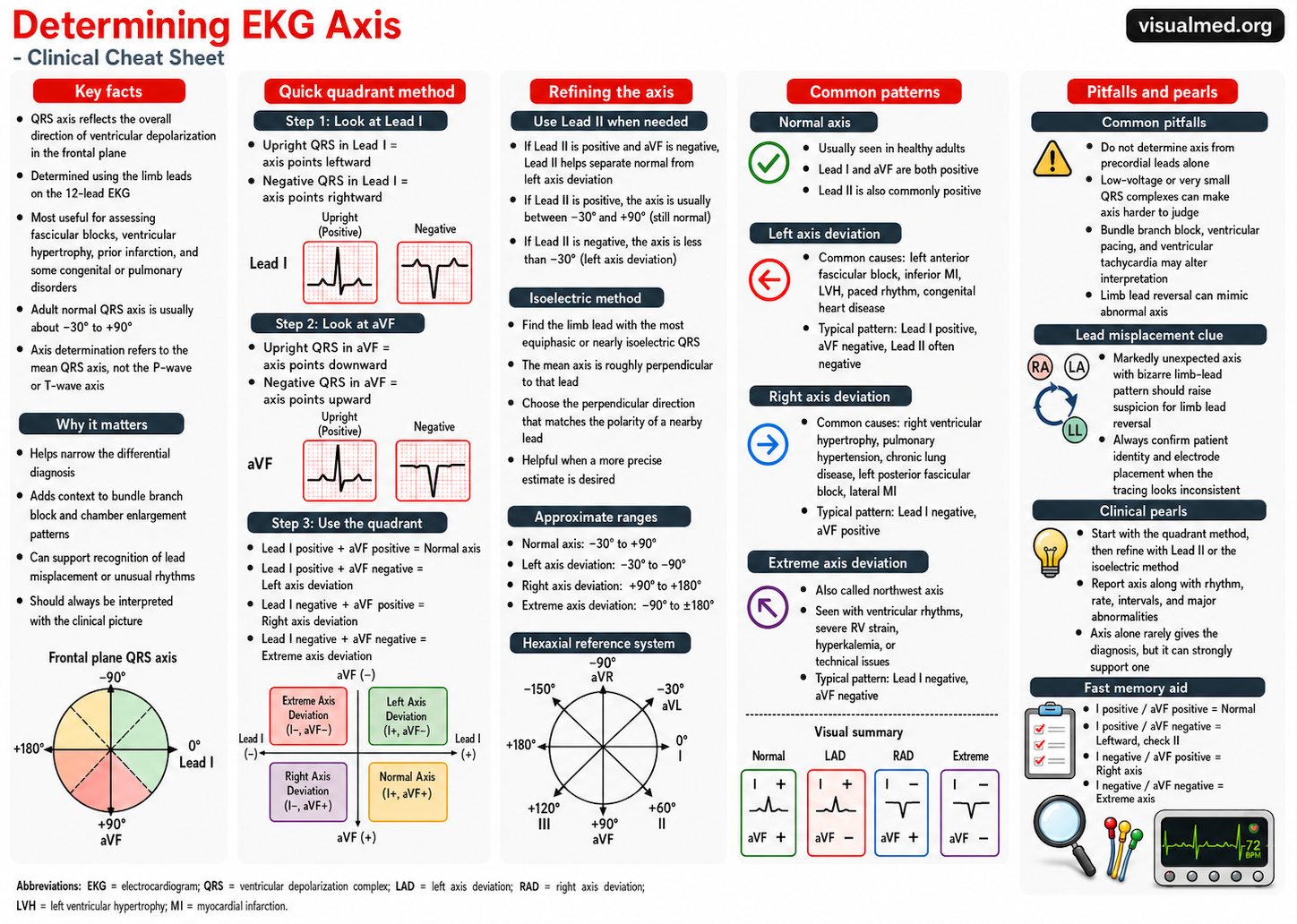
How to Determine EKG Axis: A Simple Clinical Approach
What is EKG axis? The EKG axis describes the overall direction of ventricular depolarization in the frontal plane. In practical terms, when clinicians talk about “axis,” they are usually referring to the mean QRS axis. A normal QRS axis generally points downward and to the left, because the left ventricle contributes most of the ventricular…
-
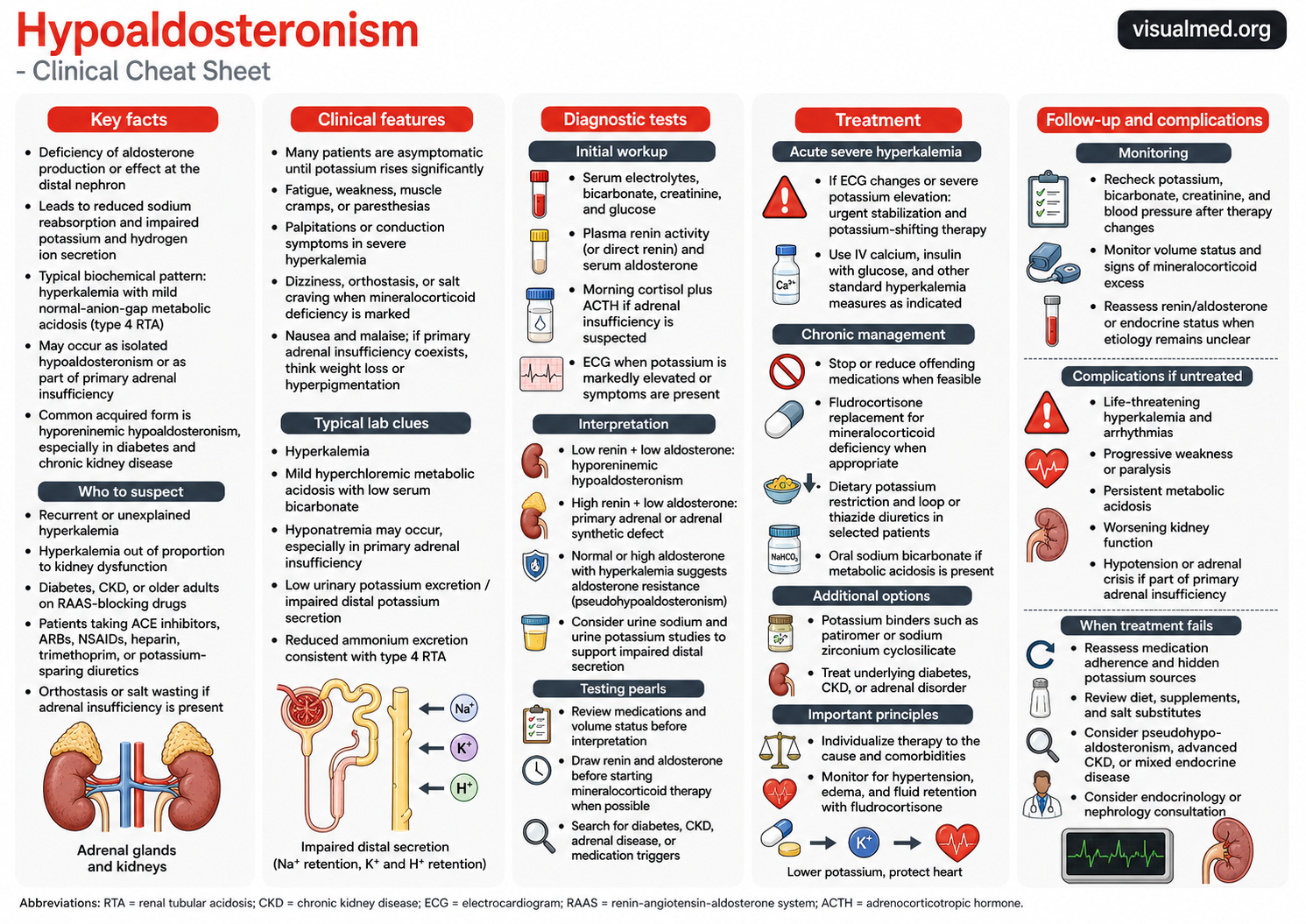
Hypoaldosteronism: Clinical Cheat Sheet
What is hypoaldosteronism? Hypoaldosteronism is a condition in which aldosterone production or aldosterone effect is reduced. Aldosterone normally acts at the distal nephron to promote sodium reabsorption and potassium and hydrogen ion secretion. When aldosterone is deficient or ineffective, patients can develop hyperkalemia and a mild normal-anion-gap metabolic acidosis, often described as type 4 renal…
-
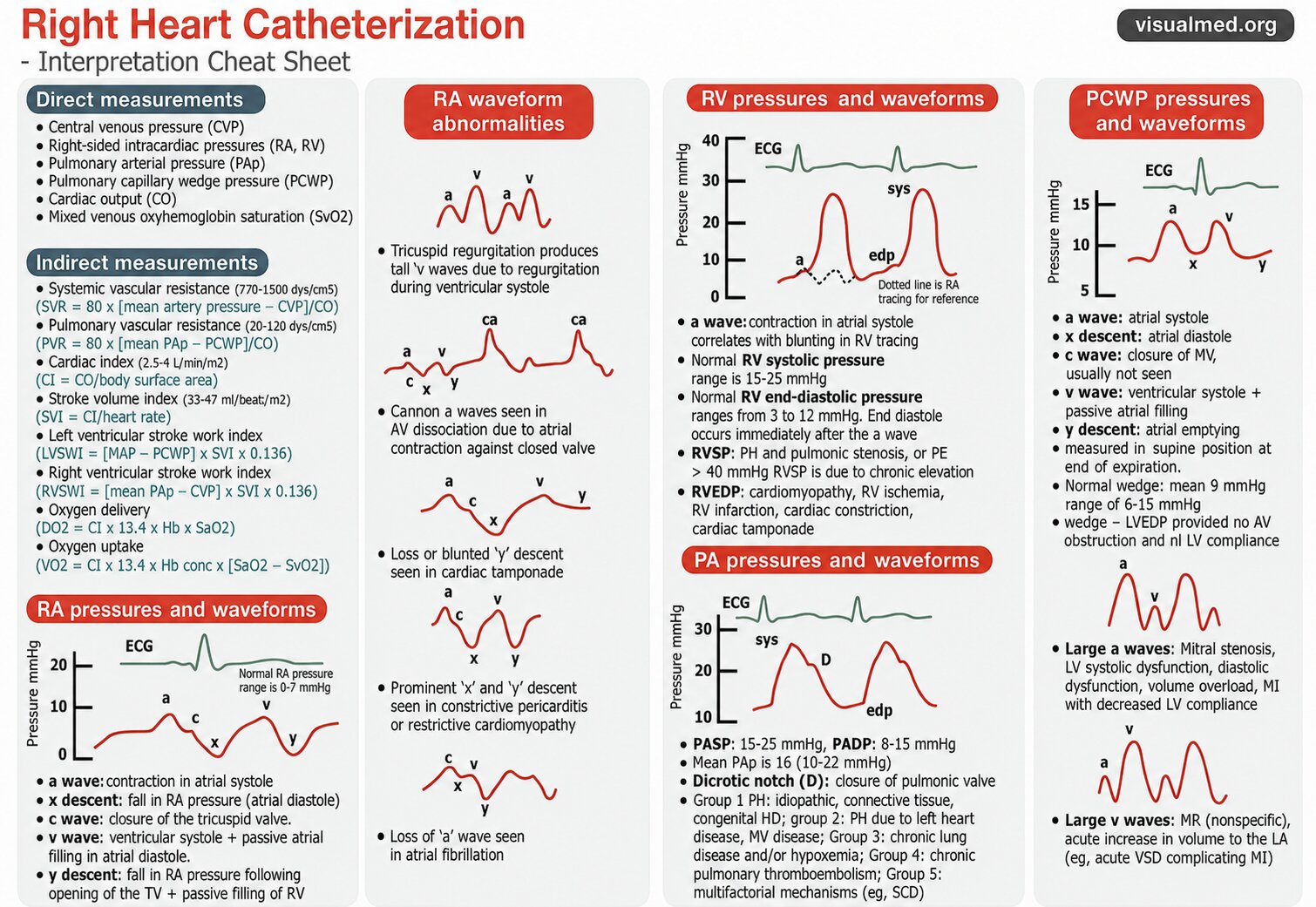
Right Heart Catheterization (RHC): Interpretation Cheat Sheet
Right heart catheterization is one of the most useful invasive tools for evaluating cardiopulmonary hemodynamics. It provides direct measurements of right-sided pressures, pulmonary artery pressures, pulmonary capillary wedge pressure, cardiac output, and oxygen saturation. When interpreted correctly, these values can help diagnose pulmonary hypertension, cardiac tamponade, constrictive physiology, valvular disease, shock states, and heart failure…
-
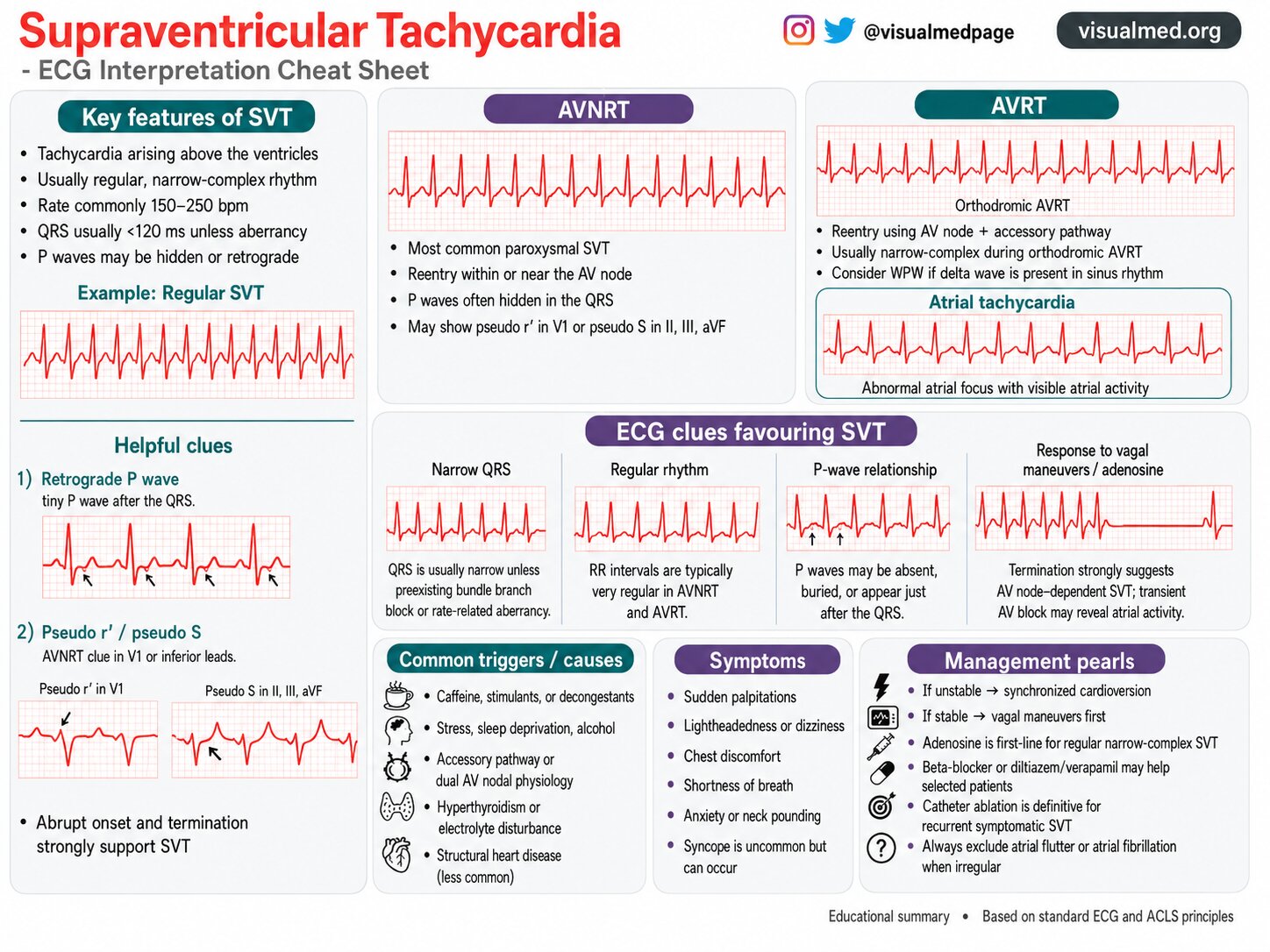
Supraventricular Tachycardia (SVT): ECG Interpretation Cheat Sheet
Supraventricular tachycardia, commonly abbreviated as SVT, refers to a group of fast heart rhythms that arise above the ventricles. These rhythms usually originate from the atria, the AV node, or an accessory pathway involving tissue outside the normal conduction system. On ECG, SVT most often appears as a regular narrow-complex tachycardia with a rapid ventricular…
-
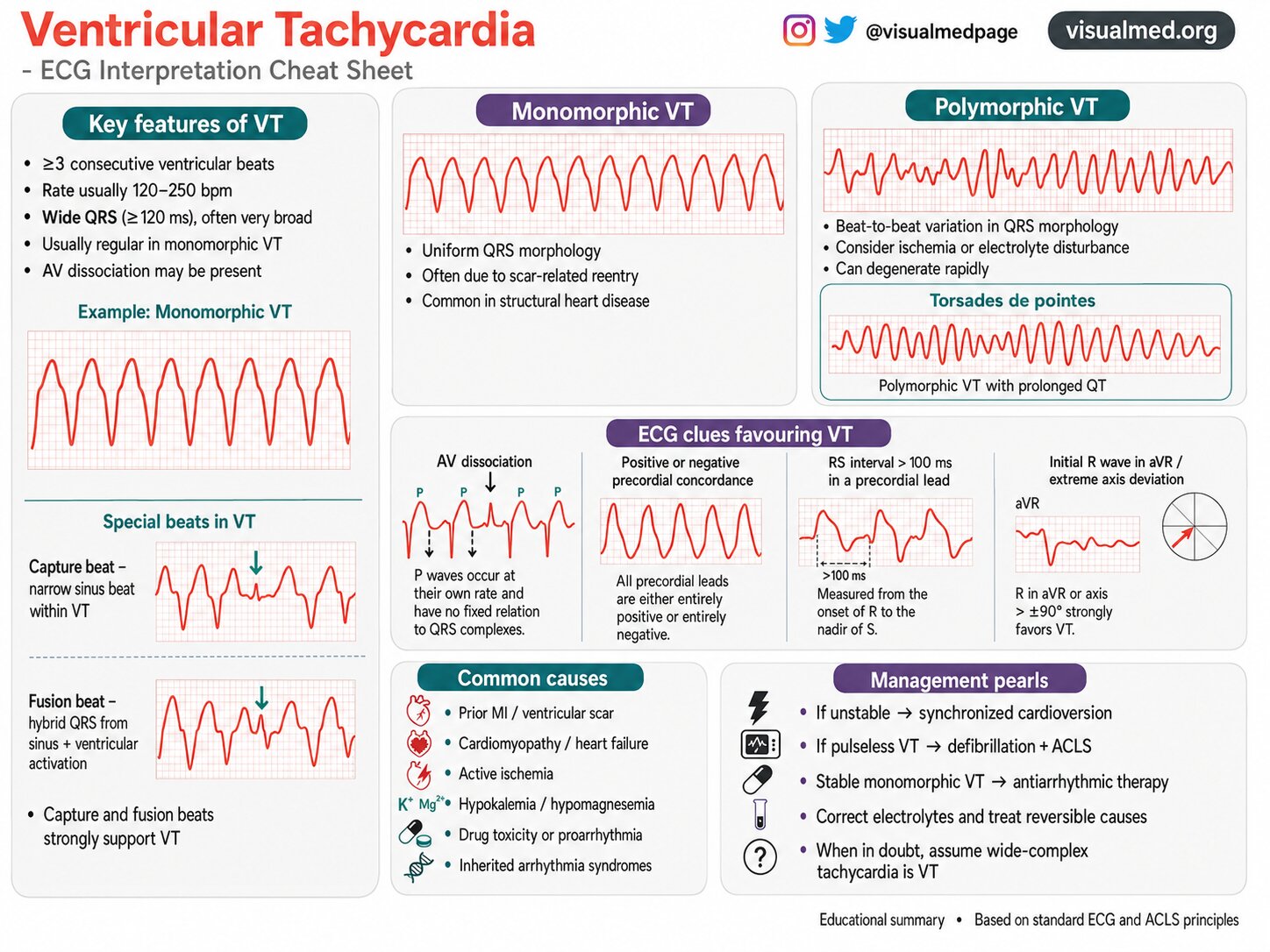
Ventricular Tachycardia: ECG Interpretation Cheat Sheet
Ventricular tachycardia (VT) is one of the most important arrhythmias to recognize on ECG. It is a potentially life-threatening rhythm that originates from the ventricles and can rapidly lead to hemodynamic collapse, cardiac arrest, or degeneration into ventricular fibrillation. Because VT often presents as a wide-complex tachycardia, prompt recognition is critical. This cheat sheet highlights…
-
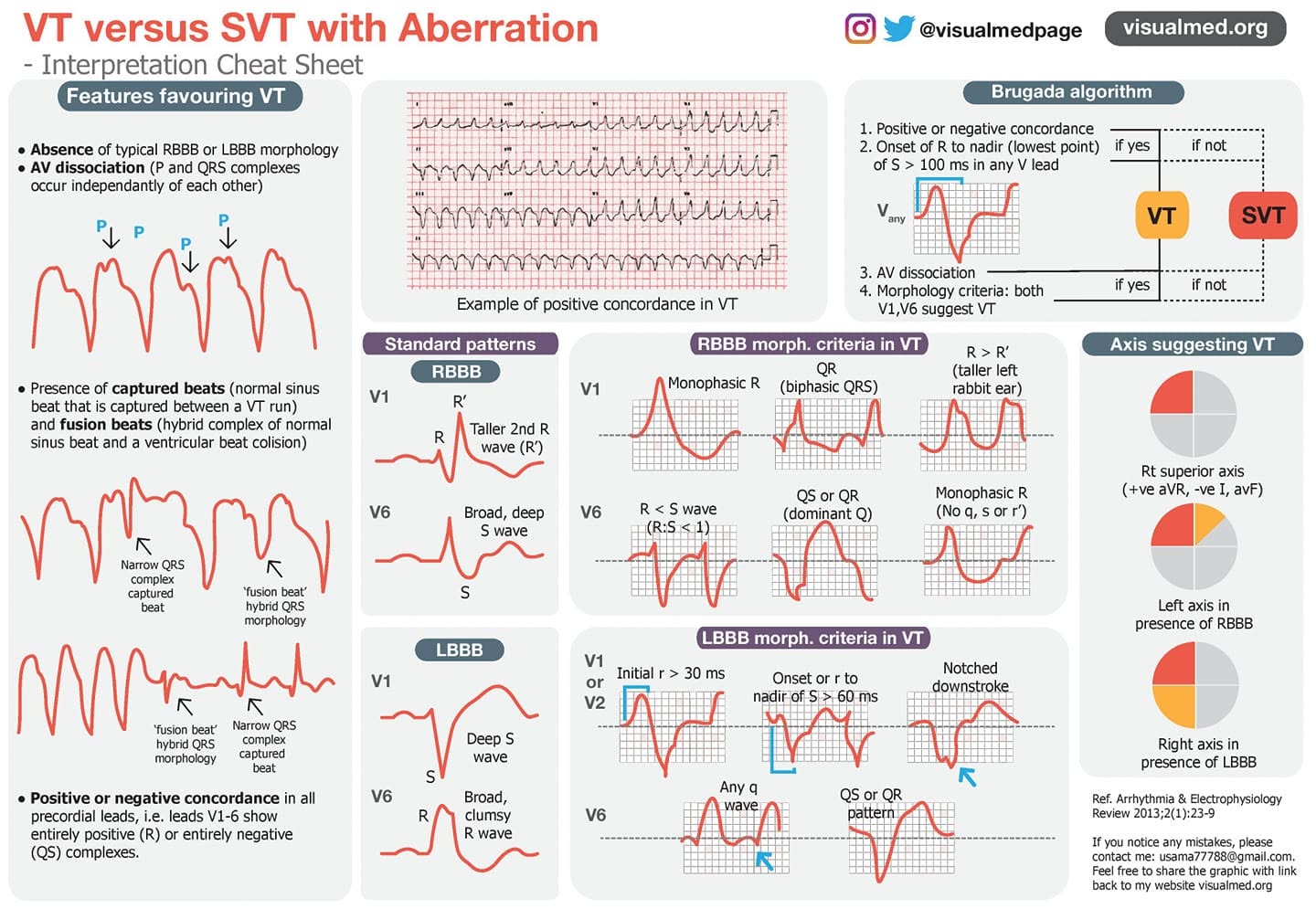
VT vs. SVT with Aberration: ECG Interpretation Cheat Sheet
Wide-complex tachycardia is one of the most important ECG patterns to recognize quickly. The key clinical question is simple: is this ventricular tachycardia, or is it supraventricular tachycardia with aberrant conduction? In practice, the safest rule is this: a regular wide-complex tachycardia should be treated as VT until proven otherwise, especially in an older patient…