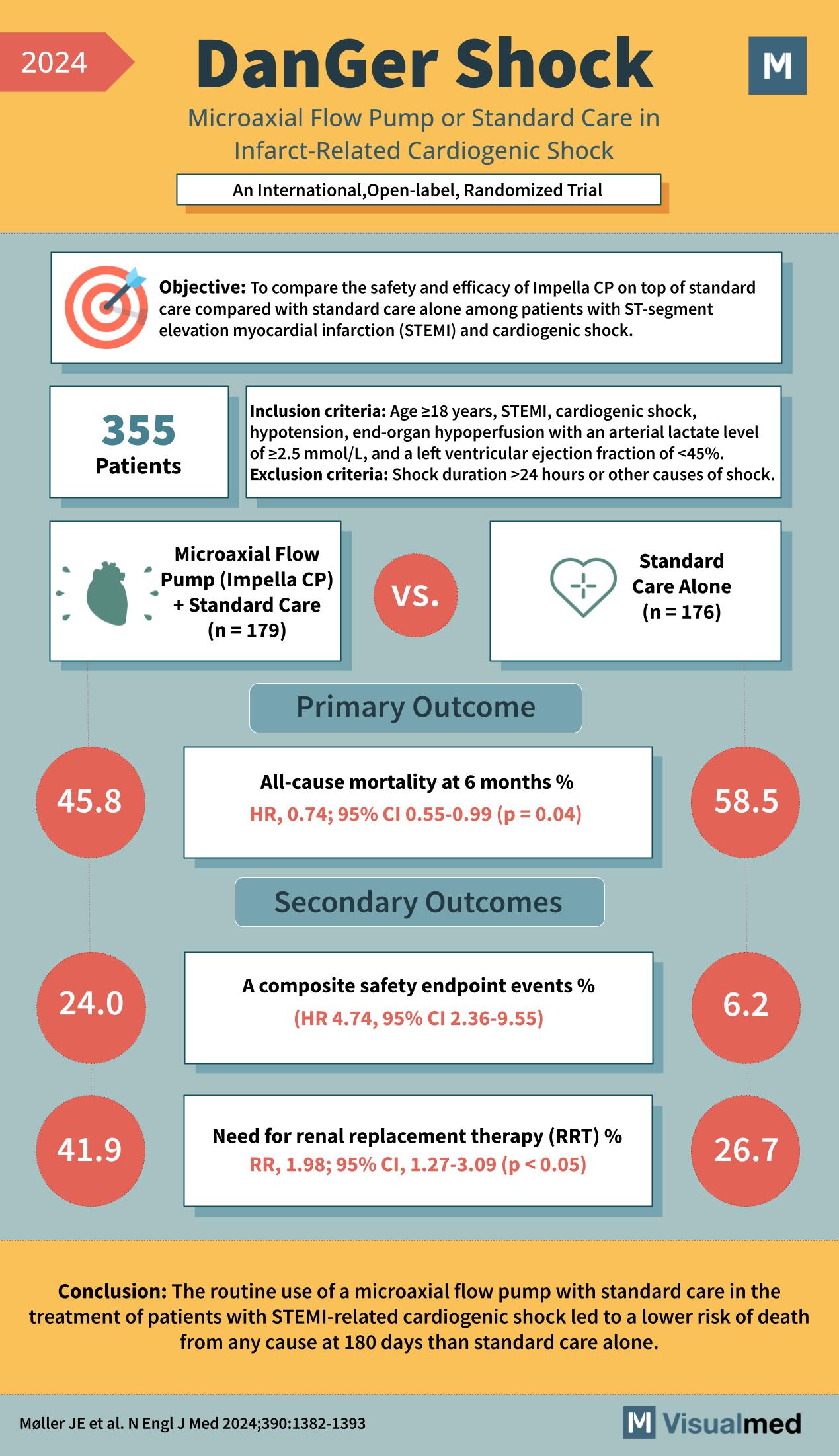
“DanGer Shock” study, which is an international, open-label, randomized trial examining the impact of a Microaxial Flow Pump (Impella CP) plus standard care versus standard care alone in infarct-related cardiogenic shock.
Objective: To compare the safety and efficacy of Impella CP on top of standard care with standard care alone among patients with ST-segment elevation myocardial infarction (STEMI) and cardiogenic shock.
Inclusion criteria:
- Age ≥18 years
- STEMI
- Cardiogenic shock
- Hypotension
- End-organ hypoperfusion with an arterial lactate level of ≥2.5 mmol/L
- Left ventricular ejection fraction of <45% Exclusion criteria:
- Shock duration >24 hours or other causes of shock.
Patients: 355 patients participated in the study.
Treatment groups:
- Microaxial Flow Pump (Impella CP) + Standard Care (n=179)
- Standard Care Alone (n=176)
Primary Outcome:
- All-cause mortality at 6 months %.
- Hazard Ratio (HR) 0.74; 95% Confidence Interval (CI) 0.55-0.99 (p=0.04)
Secondary Outcomes:
- A composite safety endpoint events % (HR 4.74; 95% CI 2.36-9.55)
- Need for renal replacement therapy (RRT) % (Relative Risk (RR) 1.98; 95% CI 1.27-3.09, p < 0.05)
Results:
- 45.8% in the Microaxial Flow Pump group experienced all-cause mortality at 6 months.
- 58.5% in the Standard Care Alone group experienced all-cause mortality at 6 months.
- 24.0% in the Microaxial Flow Pump group experienced composite safety endpoint events.
- 6.2% in the Standard Care Alone group experienced composite safety endpoint events.
- 41.9% in the Microaxial Flow Pump group required renal replacement therapy.
- 26.7% in the Standard Care Alone group required renal replacement therapy.
Conclusion: The routine use of a microaxial flow pump with standard care in the treatment of patients with STEMI-related cardiogenic shock led to a lower risk of death from any cause at 180 days than standard care alone.
Møller JE et al. N Engl J Med 2024;390:1382-1393