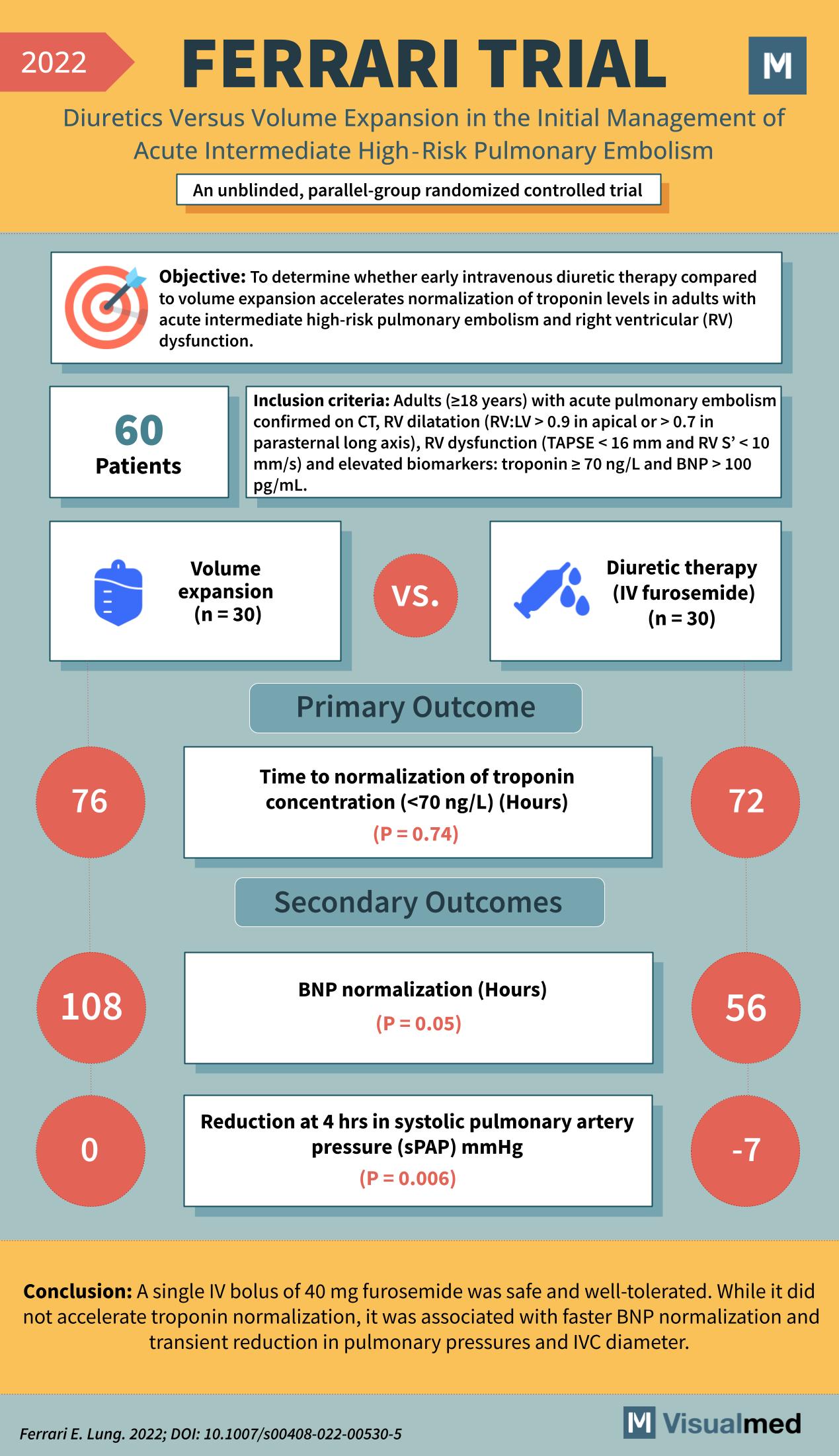
The FERRARI trial (2022) compared early intravenous diuretic therapy using 40 mg IV furosemide versus volume expansion in adults with acute intermediate high-risk pulmonary embolism (PE) and right-ventricular (RV) dysfunction. Sixty patients with CT-confirmed PE, RV dilatation, dysfunction, and elevated biomarkers (troponin ≥ 70 ng/L or BNP > 100 pg/mL) were randomized equally into the two treatment arms. The primary outcome—time to normalization of troponin levels—showed no significant difference between groups (76 h vs. 72 h; P = 0.74). However, secondary outcomes favored diuretic therapy: it led to faster BNP normalization (56 h vs. 108 h; P = 0.05) and a significant reduction in systolic pulmonary artery pressure at 4 hours (−7 mmHg; P = 0.006). The study concluded that a single IV dose of furosemide was safe, well-tolerated, and improved hemodynamic parameters without expediting troponin normalization.
Source