VOYAGER PAD Trial Summary
The VOYAGER PAD trial aimed to assess the efficacy and safety of rivaroxaban, a factor Xa inhibitor, in patients with peripheral artery disease (PAD) who had undergone lower-extremity revascularization. Patients with PAD who have undergone revascularization are at a high risk of major adverse limb and cardiovascular events, but the role of rivaroxaban in this context was uncertain.
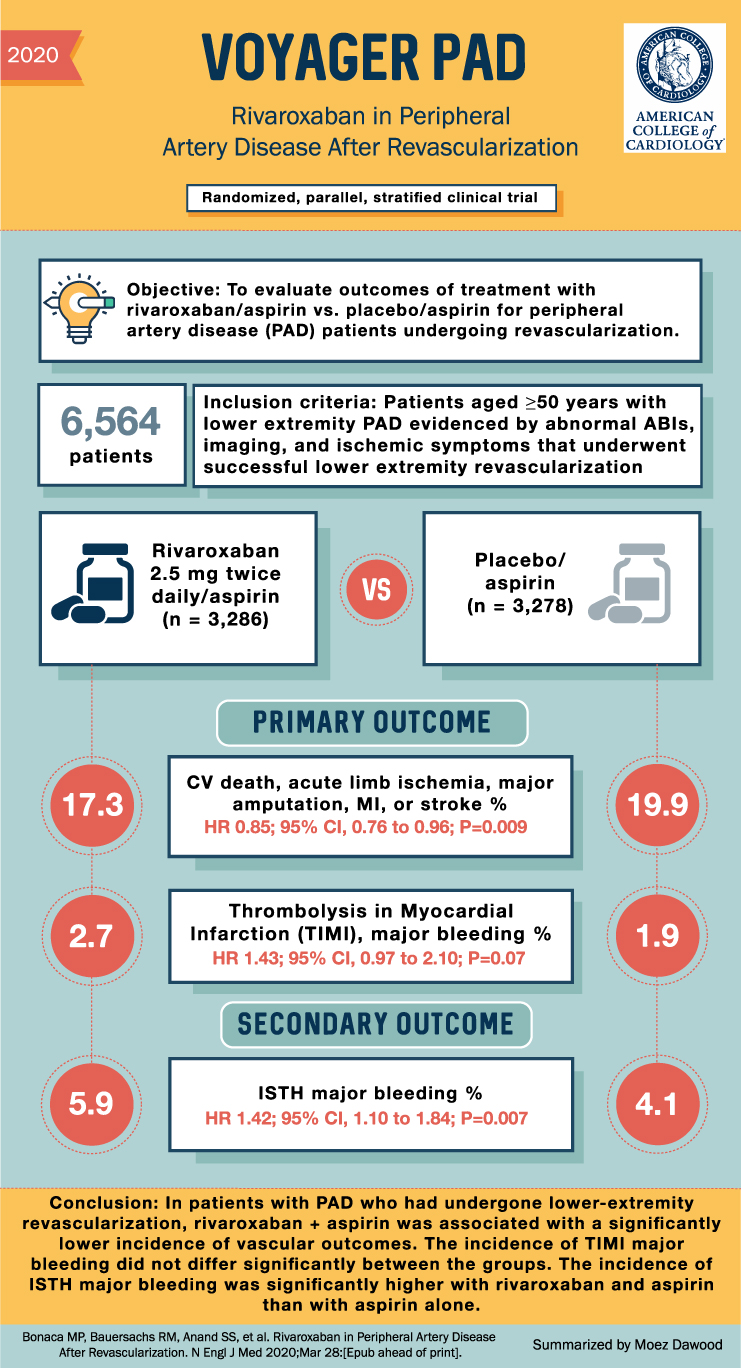
In this double-blind trial, patients with PAD and a history of revascularization were randomly assigned to receive either rivaroxaban (2.5 mg twice daily) plus aspirin or placebo plus aspirin. The primary efficacy outcome was a composite of acute limb ischemia, major amputation for vascular causes, myocardial infarction, ischemic stroke, or death from cardiovascular causes. The main safety outcome was major bleeding, defined according to the Thrombolysis in Myocardial Infarction (TIMI) classification, with major bleeding defined by the International Society on Thrombosis and Haemostasis (ISTH) as a secondary safety outcome.
A total of 6,564 patients underwent randomization, with 3,286 assigned to the rivaroxaban group and 3,278 assigned to the placebo group. The primary efficacy outcome occurred in 508 patients in the rivaroxaban group and 584 in the placebo group. The estimated incidence at 3 years, according to Kaplan-Meier analysis, was 17.3% in the rivaroxaban group and 19.9% in the placebo group (hazard ratio, 0.85; 95% confidence interval [CI], 0.76 to 0.96; P=0.009). TIMI major bleeding occurred in 62 patients in the rivaroxaban group and 44 patients in the placebo group (2.65% and 1.87%, respectively; hazard ratio, 1.43; 95% CI, 0.97 to 2.10; P=0.07). ISTH major bleeding occurred in 140 patients in the rivaroxaban group and 100 patients in the placebo group (5.94% and 4.06%, respectively; hazard ratio, 1.42; 95% CI, 1.10 to 1.84; P=0.007).
In conclusion, among patients with peripheral artery disease who had undergone lower-extremity revascularization, the addition of rivaroxaban (2.5 mg twice daily) to aspirin was associated with a significantly lower incidence of the composite outcome of acute limb ischemia, major amputation for vascular causes, myocardial infarction, ischemic stroke, or death from cardiovascular causes compared to aspirin alone. The incidence of TIMI major bleeding did not differ significantly between the rivaroxaban and placebo groups. However, the incidence of ISTH major bleeding was significantly higher with rivaroxaban and aspirin than with aspirin alone. These findings suggest that the combination of rivaroxaban and aspirin may be beneficial in reducing cardiovascular events in this patient population, but the potential risk of major bleeding should be considered when making treatment decisions.