Wolff-Parkinson-White (WPW) Syndrome
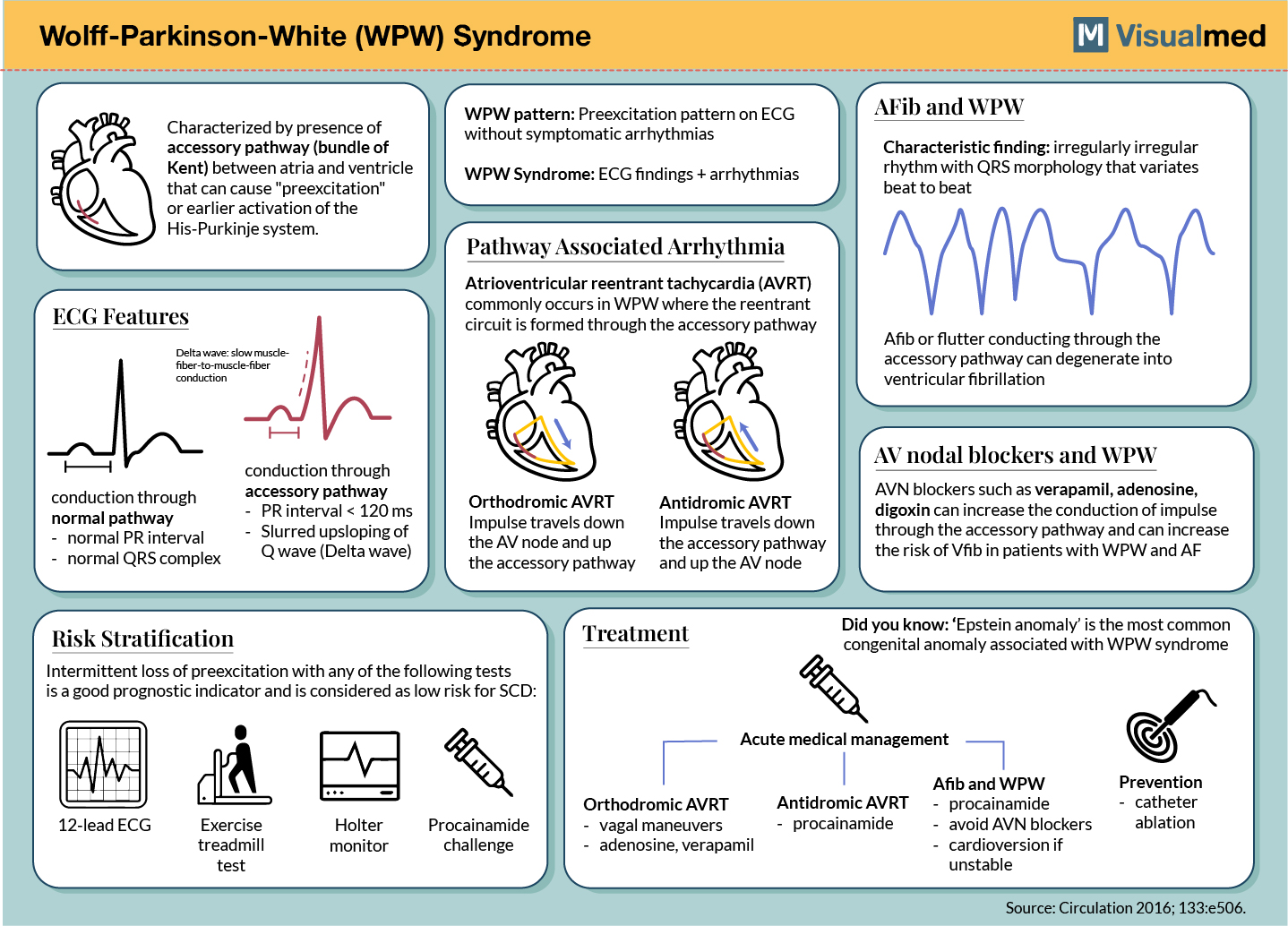
Characterized by presence of accessory pathway (bundle of Kent) between atria and ventricle that can cause “preexcitation” or earlier activation of the His-Purkinje system.
ECG Features
Delta wave: slow muscle- fiber-to-muscle-fiber
conduction
WPW pattern: Preexcitation pattern on ECG without symptomatic arrhythmias
WPW Syndrome: ECG findings + arrhythmias
Pathway Associated Arrhythmia Atrioventricular reentrant tachycardia (AVRT) commonly occurs in WPW where the reentrant circuit is formed through the accessory pathway
AFib and WPW
M Visualmed
Characteristic finding: irregularly irregular rhythm with QRS morphology that variates beat to beat
www
Afib or flutter conducting through the accessory pathway can degenerate into ventricular fibrillation
conduction through normal pathway – normal PR interval – normal QRS complex
conduction through accessory pathway
– PR interval < 120 ms Slurred upsloping of Q wave (Delta wave)
Orthodromic AVRT Impulse travels down the AV node and up the accessory pathway
Antidromic AVRT Impulse travels down the accessory pathway and up the AV node
AV nodal blockers and WPW AVN blockers such as verapamil, adenosine, digoxin can increase the conduction of impulse through the accessory pathway and can increase the risk of Vfib in patients with WPW and AF
Risk Stratification
Intermittent loss of preexcitation with any of the following tests is a good prognostic indicator and is considered as low risk for SCD:
wh
...
HM-
Treatment
Did you know: 'Epstein anomaly' is the most common congenital anomaly associated with WPW syndrome
HM-
Acute medical management
Afib and WPW procainamide
avoid AVN blockers cardioversion if
unstable
Prevention catheter ablation
Source: Circulation 2016; 133:e506.
12-lead ECG
Exercise treadmill test
Holter monitor
Procainamide challenge
Orthodromic AVRT vagal maneuvers adenosine, verapamil
Antidromic AVRT procainamide